This blog is part one of a multipart series which will review perimenopause and menopause, the history of hormone replacement therapy, the benefits of hormone therapy, current practice in hormone therapy, non pharmacological treatments, and general health guidelines for living your best in perimenopause and beyond.
Perimenopause and Menopause: An overview
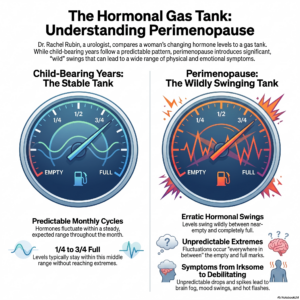
A woman has officially entered menopause once a full year has past since her last menstruation. On average a woman will live an additional 30 years past the age of menopause. Perimenopause is the transitional time leading up to menopause. It can start ten to fifteen years prior to menopause (for some women this is as early as their 30s) and is marked by a time of significant hormonal fluctuations as well as an overall decline in estrogen, progesterone and testosteron.1 Dr Rachel Rubin, a urologist who specializes in hormone and sexual health likens the changes in hormones to a gas tank. Dr. Rubin states that women in their child bearing years live with a hormonal gas tank between a quarter and three quarters tank full that predictably fluctuates throughout the monthly cycle. During perimenopause, instead of predictably fluctuating, the gas tank wildly swings from near empty to full and everywhere in between.2 To extend the analogy, when a woman enters menopause, instead of working with a gas tank, she instead has a low pilot light of estrogen, progesterone, and testosterone. Perimenopause can be further subdivided into two stages: “early transition” and “late transition.” For a woman in perimenopause, the combination of the decreasing hormones as well as the unpredictable fluctuations often lead to symptoms that can range from irksome to debilitating. For many women, perimenopausal symptoms usually become worse in the late transition period.3
Perimenopause and menopause and their associated decline in estrogen and progesterone are accompanied by a host of symptoms to include hot flushes (hot flashes), night sweats, difficulty sleeping, insomnia, difficulty concentrating, brain fog, decreased energy reserve, incontinence, more frequent urinary tract infections (UTIs), vaginal dryness, loss of sexual desire, painful intercourse, depression, anxiety, mood swings, headaches, bloating, breast tenderness, aching joints, thinning hair, palpitations, and weight gain around the abdomen.4 It is worth noting that while menopause marks the cessation of fertility, a woman in perimenopause can still become pregnant so contraception is equally important as symptom management. 2 There are a variety of pharmacological and non pharmacological options available to treat the symptoms of perimenopause and menopausal symptoms. The most recognized pharmacological treatment choice for perimenopause and menopause is hormone replacement therapy. Because scientific history plays a large role in current hormone health practices, the first part of this blog will be dedicated to reviewing the history of hormone replacement therapy.
The history of hormone replacement:
1940s- 1990s
Hormone replacement therapy was first utilized in the 1940s using a medication called Premarin. Premarin is a synthetic estrogen whose name derives from the fact that it was created from the urine of pregnant mares.2 There was an explosion of Premarin prescriptions when in the 1960s, Dr. Robert Wilson published a book titled “Forever Feminine” in which menopause was labeled as a “living decay” as opposed to a natural process. 4 “Forever Feminine” is now widely viewed as a remarkable piece of medical misogyny in which hormone replacement therapy was touted as a fountain of youth and a means to preserve femininity. The underlying message was that estrogen replacement could make a woman appear more attractive, increase her interest in sex, and make her less bothersome to her husband. Printed at the time of rising feminism, it created a divide among women. Some viewed hormones as a means for more comfortable living. Others viewed hormones as another tool of the patriarchal oppression.5 Later it was revealed that Dr. Wilson’s foundation and book were secretly funded by Wyeth, the pharmaceutical manufacturer of Premarin. With the explosive use of Premarin came an uptick in uterine cancer and the realization that unopposed estrogen increased the risk of uterine cancer. At this point, Premarin was combined with a synthetic progestin called Medroxyprogesterone Acetate in order to protect the uterus.4 In combination these two drugs were called Prempro. It is important to note that hormone therapy today utilizes bio-identical hormones as opposed to synthetic hormones. This will be discussed in further detail later.

The Women’s Health Initiative:
In 1998 the National Institute of Health (NIH) funded the billion-dollar Women’s Health Initiative (WHI). The WHI was the largest prospective study ever done of women’s health. The primary goal of the study was to measure the effects of hormone therapy on coronary artery disease (CAD) and to observe if hormone therapy reduced the risk of CAD. Secondary data points included blood clots in the legs also known as deep vein thrombosis or DVTs, blood clots in the lungs, also known as pulmonary emboli or PEs, breast cancer, Alzheimer’s disease, dementia, fractures, type 2 diabetes mellitus (T2DM), all cause mortality, weight gain, bone mineral density, joint pain, stroke, glaucoma and more.6 The average age of the women in the study was 62 and it studied women up to 79 years old.2 Women with a uterus were prescribed a fixed dose of conjugated combined hormone therapy (Prempro). Women without a uterus were prescribed a fixed dose of conjugated estrogen only therapy (Premarin). 6
In 2002, a few years into the study, the National Institutes of Health issued a press release that stated “The NIH has stopped early the Women’s Health Initiative… due to an increased risk of invasive breast cancer.” Shortly thereafter and prior to actually publishing the research, the Journal of American Medical Association (JAMA) added that Prempro not only increased the risk of breast cancer, it also increased the risk of coronary heart disease, stroke, and blood clots.4 This headline was shocking. Millions of women on hormone replacement were suddenly inundated with alarming headlines on the seemingly unmitigated dangers of hormone therapy. It is important to note that publication by press conference should raise at least eyebrows if not actual red flags. When publishers provide jaw dropping sound bites prior to publishing the research in total, it prevents reporters, scientists, and physicians from examining the researchers’ findings, and all but guarantees that the attention grabbing headlines will be what people remember the most.
When the study was finally published eight days after the headlines, there were some medical professionals and statisticians noting flaws in statistical design, however their objections were largely drowned out by the cacophony of shocking results. It is also important to point out that the initial results submitted to JAMA were done so without informing all the principle investigators- another eyebrow raising move in the scientific community. 4 One epidemiologist who had been part of the WHI, Dr. Robert Langer, stated that many principle investigators had seen the paper only after it had been accepted at JAMA, and “concerns were raised about the tone, the analysis conducted and reported, and the interpretation of the results in the paper.”7 This whole process goes against academic norms: there were concerns with statistical accuracy, there was an incomplete principle investigator review, and press release and publicity occurred prior to publication.
There are thousands of pages in books and articles that thoroughly review some of the flaws behind the results of the WHI. Below are some noted study limitations as well as under reported benefits among the WHI’s findings.
Breast cancer
The WHI results showed that women in the estrogen alone group had a decrease incidence of being diagnosed with breast cancer and of dying of breast cancer compared to the placebo group. Interestingly, this finding did not receive public attention. In contrast, the women taking combined hormone therapy were reported to have an increased risk of being diagnosed with breast cancer but not an increased risk of dying of breast cancer compared to the placebo group.8
There are a few issues with how these results were interpreted and reported. First, the placebo group was not a true or “clean” placebo group. Further analysis showed that the initial results did not fully adjust for women who had previously used hormone therapy. A large percentage of the women in the placebo group had been on previous hormone therapy and this subgroup was found to have an unusually low risk of breast cancer. This made the combined hormone replacement group appear riskier by comparison. When the women with prior exposure to hormone therapy were removed from the placebo group, the difference in the risk of breast cancer and dying of breast cancer between the placebo group and the combined hormone group were no longer evident.2,4,9
The second issue is how risk is reported. The initial WHI results emphasized relative risk and hazard ratio, which can make findings sound more alarming. Absolute risk is the actual chance of something happening. This tells you how common (or uncommon) something really is. For example, if 100,000 people are eating bagels and 2 of those individuals choke on the bagel then the absolute risk is 2 in 100,000. Similarly, if 100,000 people are eating a croissant and 4 of those individuals choke on the croissant then the absolute risk is 4 in 100,000. Relative risk on the other hand compares one situation to another. Relative risk answers the question of how much does the risk change. Using the same example, if 2 in 100,000 people choke while eating a bagel compared to 4 in 100,000 people who choke while eating a croissant, then the relative risk of chocking on a croissant is double that of choking on a bagel. This is why relative risk can sound dramatic without showing how uncommon the event was to begin with.
To put a little simpler, in the WHI study, the chance of a woman developing breast cancer in the placebo group was 4 in 1,000. The chance of woman developing breast cancer in the combined hormone group was 5 in 1,000. As a relative risk this is a 25% increase. As a calculated absolute risk this is a 0.08% increase.1
Similarly, a hazard ratio is a way that researchers compare how often an event happens over time in one group or another. The WHI reported a hazard ratio of 1.26 for breast cancer among those receiving combined hormone therapy versus the placebo group which “almost reached nominal statistical significance.”11 In other words, the reported increase in breast cancer risk was a relative measure, and even by the researchers’ own word choice, it was at best borderline significant rather than clearly statistically significant. This distinction matters because the public messaging around the WHI often presented the risk as more definitive and more clinically alarming than the data supported.
Blood clots in legs and lungs:
There was a reported risk in blood clots in the legs and lungs in both the combined hormone and estrogen only groups8. Recall that the average age of the women receiving these synthetic hormones was 62 years old. Also recall that the WHI was conducted with synthetically derived hormones as opposed to the currently used bioidentical hormones. Oral contraception is derived from synthetic hormones. A known risk of oral contraception is blood clots, and thus it is no great surprise that women in their 50s, 60s, and beyond were developing blood clots while on synthetic hormones. However, as previously stated, most current practices no longer utilize synthetic hormones, and instead focus on the use of bio-identical estrogen, progesterone, and in some cases, testosterone. What’s more, current hormone replacement replaces systemic estrogen in the form of patches, creams, and gels, thus avoiding the first pass effect in the liver and mitigating the risk of blood clots even in those prone to blood clots. Lastly, to again paraphrase Dr. Rachel Rubin, to state that bioidentical hormones should be avoided because synthetic hormones increase the risk of blood clots is like saying an individual should avoid eating strawberries because strawberry flavored gummy bears are bad for one’s health.2 They are not the same.
Other WHI findings
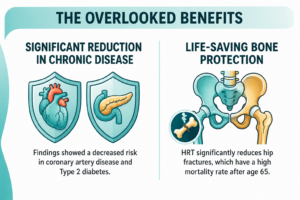
On the other hand, the WHI did reveal a number of meaningful benefits to those taking the combined and estrogen only therapies. These benefits included a decreased risk in coronary artery disease (contrary to the press release), type 2 diabetes, fractures, especially hip fractures, and death from any cause.8 Hip fractures are a particularly important point of evidence. Hip fractures that occur in people over 65 are associated with a 27% chance of death within the year, and a 79% chance of death within 9 years. A hip fracture, even if it does not result in death, does come with a significant reduction in quality of life which is why strength training, mobility exercises, and a diet rich in calcium and vitamin D is so important.11
Part Two: Beyond the WHI
Stay tuned for part two of the hormone health blog which will take a deeper look at the benefits of hormone therapy (its more than just symptom management!) current practices used at The Coit House including hormone therapy, nonhormonal treatment options, and lifestyle recommendations to support overall health during the perimenopause years and beyond.
Authored by Megan Heimerl, FNP.
Schedule an appointment for Hormone Health & Wellness at The Coit House
Reference List
- Haver, M.C. (2026). The new perimenopause: An evidence-based guide to surviving the zone of chaos and feeling like yourself again. Rodale Books.
- Rubin, R. S. (n.d.). Hormone therapy for early adopters on-demand [Online course]. Rachel Rubin MD. https://rachelrubinmd.thinkific.com/courses/MHTCME
- Shah, A. (2026). Hormone Havoc. Harper Colins.
- Bluming, A. Z., & Tavris, C. (2024). Estrogen matters: Why taking hormones in menopause can improve and lengthen women’s lives—without raising the risk of breast cancer (Rev. & updated ed.). Little, Brown Spark.
- Houck, J. A. (2003). “What do these women want?” Feminist responses to Feminine forever, 1963–1980. Bulletin of the History of Medicine, 77(1), 103–132. https://doi.org/10.1353/bhm.2003.0023
- The Women’s Health Initiative Study Group. (1998). Design of the Women’s Health Initiative clinical trial and observational study. Controlled Clinical Trials, 19(1), 61–109. https://doi.org/10.1016/S0197-2456(97)00078-0
- Langer, R. D. (2017). The evidence base for HRT: What can we believe? Climacteric, 20(2), 91–96. https://doi.org/10.1080/13697137.2017.1280251
- The North American Menopause Society. (2022). The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 29(7), 767–794. https://doi.org/10.1097/GME.0000000000002028
- Bluming, A. Z., Hodis, H. N., & Langer, R. D. (2023). ‘Tis but a scratch: A critical review of the Women’s Health Initiative evidence associating menopausal hormone therapy with the risk of breast cancer. Menopause, 30(12), 1241–1245. https://doi.org/10.1097/GME.0000000000002267
- Writing Group for the Women’s Health Initiative Investigators. (2002). Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative randomized controlled trial. JAMA, 288(3), 321–333. https://doi.org/10.1001/jama.288.3.321
- Panula, J., Pihlajamäki, H., Mattila, V. M., Jaatinen, P., Vahlberg, T., Aarnio, P., & Kivelä, S.-L. (2011). Mortality and cause of death in hip fracture patients aged 65 or older: A population-based study. BMC Musculoskeletal Disorders, 12, Article 105. https://doi.org/10.1186/1471-2474-12-105
